Opening notes
Dear Black family,
In deciding to write this essay, I had to dig very deep into my own experiences and emotional reserves and so, if you detect any inconsistencies or incoherence, please accept my sincere apologies. I realise this essay might be a bit longish for some, but I humbly request that you take the time to read it and hopefully it will nudge you to do some further reading of your own (that is if you have not already done so), on the subject of depression and mental disorders in general.
This essay doesn’t in anyway claim to be comprehensive and neither should it be construed as professional medical advice. The reader is urged to all times seek professional medical advice, on depression and related subjects. The primary purpose of this essay is to ignite a critical reflection and hopefully deepen our understanding of the challenge of depression in the Black community (a focus that the author has and will never apologise for).
The issue of depression has become very much topical lately in South African media (traditional and new), and the unfortunate passing of our Brother and Motswako icon, Jabulani Tsambo aka HHP, just brought the issue of depression into even sharper public focus. However, depression is actually an everyday problem that affects all Black people, regardless of their social status or bank balance.
By virtue of my various leadership roles, I regularly find myself in the position where I have to sit and listen to a Black Sister or Brother, sharing very intimate details about the various issues that are troubling them. A lot of times, it gets so overwhelming that the people (men and women), who request my audience, just break down in front of me. There are also moments where I also breakdown.
Even though I have no formal training as a counsellor or therapist, I find myself in these situations almost weekly and in spite of being aware of my capacity limitations, I find it extremely difficult ( if not a lack of compassion), to turn such people away and direct them elsewhere, especially if they specifically request to speak to me. I suspect many of us (even those who hold no formal leadership positions), often find themselves in situations where they have to be the proverbial shoulder to lean on.
But do we know the actual source of the personal problems that we and others are wrestling with every day? Those who follow me on Facebook will recall that I recently posted a couple of times on the subject of depression and even went as far to suggest that, many of us (Black people) may be unknowingly suffering from depression. Unsurprisingly, my post ignited a very lively debate, which I hope will continue.
Informed by how I look at the world and as stated above, I am interested in the impact of depression on the Black community and in particular, the mental health of this community. There are at least four factors that inform my focus. One, the debilitating persistence of violence and in particular inter-personal and gendered violence in the Black community. The murder of 14 year-old Valencia Farmer in June 1999, remains forever ingrained in my mind.
As some of you know, young Valencia was gang raped, stabbed more than 50 times and her throat was slit. She was left for dead in a derelict house in Eerste River. Naked and seriously injured, Valencia managed to crawl to the street, where neighbours found her. She later died in hospital, after she was able to mumble the names of her attackers.
Two, the alarmingly high participation rate of Black men (and especially young people) in acts of violence and in particular the rate at which they are incarcerated. For instance, the young men who attacked Valencia, were aged 16, 19 and 20 at the time. According to the data from the Department of Correctional Services, South Africa’s prison population is at over 160 000.
97% are male prisoners and a frightening 125 006 or 79.6% are Blacks. In 2017, there was a reported overcrowding rate of 149%, with Pollmoor Prison having the highest of bed shortages with 2448, for the financial year 2015/16.
Three, the disturbing phenomenon of teenage suicide. According to the South African Depression and Anxiety Group (SADAG), “the incidence of suicide in South Africa has soared to 23 a day.” And four, I am also interested in the impact of general structural factors such as the persistence of economic inequality on the general mental health of the Black community.
According to Statistics South Africa, “the unemployment rate in South Africa increased to 27.2 percent in the second quarter of 2018 from 26.7 percent in the previous period. The number of unemployed rose by 103 thousand to 6.08 million while the number of employed fell by 90 thousand to 16.29 million.”
Statistics South Africa further states that, “South Africa remains a dual economy with one of the highest inequality rates in the world, perpetuating both inequality and exclusion. The Gini coefficient measuring relative wealth reached 0.65 in 2014 based on expenditure data (excluding taxes), and 0.69 based on income data (including salaries, wages, and social grants). The poorest 20% of the South African population consume less than 3% of total expenditure, while the wealthiest 20% consume 65%.”
But I must also admit, my interest in informing myself on the subject of depression also arises out of the suspicion that I may well be part of those who are unknowingly suffering from depression. If a professional confirms this, I won’t be surprised.
WHAT IS DEPRESSION?
Depression is generally described as “a mental health disorder characterised by persistently depressed mood or loss of interest in activities, causing significant impairment in daily life.” Other mental disorders include bipolar affective disorder, schizophrenia and other psychoses, dementia, intellectual disabilities and developmental disorders including autism.
In trying to help us understand the global impact of depression and its characteristics, the World Health Organisation makes the following observations:
- Depression is a common illness worldwide and globally, more than 300 million people of all ages suffer from depression;
- It is the leading cause of disability worldwide;
- It is a major contributor to the overall global burden of disease;
- It affects women more than men;
- At its extreme stages, depression can lead to suicide;
- Globally, about 800 000 people die due to suicide every year; and
- Suicide is the second leading cause of death among 15-29-year-olds.
WHAT ARE SOME OF THE SIGNS OR SYMPTOMS OF DEPRESSION?
According to the June 2017 edition of the Natural Medicine Magazine, some of the signs and symptoms of depression are the following:
- Feeling sad, anxious or ’empty’ most of the time.
- A loss of interest or pleasure in hobbies and activities that were once enjoyed.
- Feeling hopeless about life and feeling helpless or guilty.
- A depressed person experiences changes in sleeping habits -they sleep more than usual or sleep less.
- They gain a lot of weight or lose a lot.
- They feel slow or fatigued.
- They experience restlessness, irritability, anger and difficulty concentrating.
HOW CAN YOU DEAL WITH DEPRESSION?
The Natural Medicine magazine referred to earlier, also states that, therapy and antidepressants are considered to be the most effective treatments for depression, however the following at - home ways for dealing with depression, are recommended:
- Follow a routine: Get out of bed and get dressed every day.
- Schedule time for relaxation – read, listen to music, paint or watch television.
- Remember the things you once enjoyed doing – even if you just spend 15 minutes doing these activities.
- Set goals: Keep them simple and realistic. It is possible that you are not well enough to do your daily tasks, but do what you can and don’t beat yourself up if you fail.
- Exercise: Any form of exercise, however small, is beneficial. Exercise gives you much needed ‘feel-good’ brain chemicals.
- Eat well and avoid unhealthy habits: Eat small snacks and not large meals. Drink lots of water. Water gives energy. Avoid drugs and alcohol.
- Get a good night’s sleep: If you have trouble sleeping, avoid exercise and caffeine after 17:00 and steer clear of non-prescription sleeping pills. If needed, ask your doctor for something to help you sleep.
- Educate yourself: Learn as much as you can about your illness. Give related books to friends and family so they can understand what you are experiencing.
- Keep a journal: Write your feelings down. It will help to put things into perspective.
- Don’t do anything rash: Avoid making big decisions, such as changing jobs or moving house, until you feel better.
- Honour achievements: Acknowledge the small goals you meet every day.
- Join a support group: It is liberating to go somewhere you can talk and no one judges. It also serves as a place to get great advice.
- Do volunteer work: Help others. Go to a school, hospital, an old age home or hospice and find out what they need. Remember that you are important in your community.
- Healing takes time: Don’t give up on treatment – it can take two to four weeks for antidepressants to have an effect on symptoms.
WHAT IS THE SOUTH AFRICAN SITUATION?
According to the South African Depression and Anxiety Group (SADAG), a non-profit organisation that has been doing work in the area of depression and related mental disorders since 1994, the South African situation is characterised by among others, the following:
- In South Africa, like in many other developing countries, mental health doesn’t feature as a public health priority, and in rural communities mental health is not supported at all;
- 20% of all South Africans will experience a depressive disorder at least once during their lifetime;
- 21.4% of teenagers in South Africa have considered committing suicide due to a combination of issues including relationship problems, trauma for various reasons including but not limited to family issues, violence, emotional or sexual abuse, bullying, substance abuse, teenage pregnancy and exam stress. Many learners are affected by peer pressure to use alcohol, start smoking and use drugs at early ages;
- 60% of teenagers do not seek assistance, mainly because they do not know that there are resources available;
- Young people between the ages of 19 and 24 are considered to be the most at-risk group for depression and suicide;
- 20% of university students have suicidal thoughts at some point during their university career ; and
- 90% of student suicides are found to have a psychiatric diagnosis. Student suicides is an area that deserves urgent attention.
WHAT IS THE RELATIONSHIP BETWEEN DEPRESSION AND SUICIDE?
From the data of the World Health Organisation and the SADAG, there is a clear correlation between depression and suicide. The suicide of celebrated Black professor, Bongani Mayosi of the University of Cape Town and those of students at the universities of Rhodes, Johannesburg and recently, Wits point to the seriousness of depression-induced suicide in South Africa.
According to the organisation, Africa Check, South Africa’s suicide profile has the following characteristics:
- In 2012, there were 6133 suicides in South Africa (this is from the Medical Research Council’s Burden of Disease Study);
- Statistics South Africa’s 2015 Mortality and Causes of Death report estimated that 484 deaths were due to self-harm. The statistics are based on death certificates from the department of home affairs, but experts caution that suicide deaths are under-reported on these forms;
- The vast majority of suicides victims in South Africa are male. 14 men all of ages died by suicide every day;
- In 2012, 5,095 men of all ages died due to suicide – equalling nearly 14 each day. This is lower than the frequently reported statistic that 18 men die due to suicide every day in the country;
- The male death rate for suicide was 21 per 100,000 people, over 5 times higher than the female death rate by suicide of 4;
- White men have a higher suicide rate. A racial breakdown of the Medical Research Council’s suicide statistics reveals that white men have the highest suicide rate in the country;
- For every 100,000 white men in South Africa in 2012, 30 white men died as a result of suicide. This was 2.5 higher than the national suicide death rate of 12 and 1.4 times higher than the national male suicide rate;
- Suicide is the 4th leading cause of death for young people;
- Suicide was the fourth leading cause of death for young people aged 15-24 in South Africa in 2012. That year, 1,665 young people died as a result of suicide. AIDS-related illnesses were the leading cause of death (6,822 deaths) followed by interpersonal violence (5,359) and road injuries (2,950);
- The World Health Organization (WHO) estimated that there were 12.3 deaths by suicide for every 100,000 people in South Africa in 2015. At this rate; and, South Africa didn’t even feature in the top 50.
NB: It is important to note that the WHO strongly advises against drawing any international comparisons using suicide rates. This is because suicide can be under-reported to varying degrees in different countries.
CONCLUDING NOTES
From the investigation I have done, it seems to me there is an urgent need for activist Black knowledge workers to produce easily-accessible activist-type research on the subject of depression and its impact on the general mental health of the Black community.
I often find that, even in institutional academic research, there is rarely a deliberate interest in focusing on the critical issues facing the Black community. This is also why you sometimes find that state-policy interventions being influenced by research that is based on the experiences of countries whose history has little or nothing in common with that of South Africa.
SADAG makes a related but equally-problematic observation that “Although the prevalence of depression amongst black South Africans is largely un-investigated due to problems relating to language and cultural differences, the studies that have been done indicate that the numbers are seriously high, with approximately 18% of black patients presenting at primary health care facilities being found to be suffering from depression. This may even be an underestimation of the figures, as it has been found that GP's fail to detect between 33% to 50% of depressive disorders in patients presenting to them.”
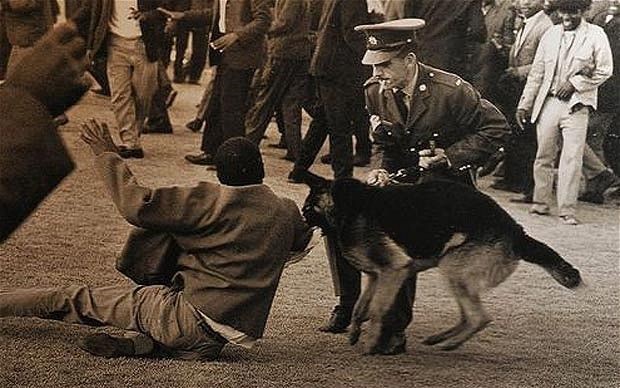
As a result of our history of European invasion, imported white-violence and consequent powerlessness, as a Black child your whole being is shaped by a pressure-cooker type environment that is characterised by a high prevalence of assault, rape (especially of children), robbery, murder (especially of women), gang violence (particularly on the Cape Flats), drug and alcohol abuse, the frightening number of Black young men in prison, a high number of single-parent, child-headed or single-income households and chronic unemployment.
Then there is also the individualised trauma that comes from losing a loved-one (especially a partner or child), experiencing divorce, having a miscarriage (s), being betrayed or abused by a loved-one, close friend or relative, having to deal with the reality of being disabled or raising a child with one or the other disability, being diagnosed with a life-threatening illness, high levels of indebtedness, being declined for poor credit by business institutions.
Losing a job or a huge sum of money, having your house or car repossessed by a bank, being bullied by an abusive manager at work, the frustration of not having money to further your studies or sitting with a mountain of certificates and no job, the trauma of being trapped in a concentration camp (township). And to compound all this, then you are also up against a sophisticated machinery of state policies that are more concerned with the needs of the markets and not your basic aspirations as a Black person.
If you consider all of this and the collective impact on the mental health of the individual Black person, it becomes clear (of course not to every Black person) that every day, as a Black person, you have to contend with multiple layers of violence (seen and unseen). This explains why we are generally edgy and ready to lash out at each other, at the slightest instigation.
How do we expect Black young girls and boys to grow up to become normal, functional and productive members of society, in such a toxic, debilitating and disempowering environment? And if you struggle to relate to what I am describing, I invite you, dear reader, to please make time and pay a visit to hell-holes such as Town Two in Khayelitsha, Eziphunzana in East London or Diepsloot in Johannesburg.
If SADAG’s observation is anything to go by, then the problem facing the Black community is much bigger than depression. While we are waiting for the research by activist Black knowledge workers, there are certain practical things I believe the Black people of my generation must do. One is to use our access to the internet more meaningfully and gather as much information on depression and related mental illnesses as possible.
The other is to set up or join support groups where we stay or work. I have already initiated one for men. If you need further assistance, SADAG has a nationwide-reach and offers a variety support services, advice and training on how to deal with depression and related mental disorders. I therefore recommend you contact the SADAG, through the contact details provided below.
Finally, I hope my clumsy reflections inspire you to do more reading on depression and related mental disorders. Most importantly, I hope I have inspired you to act, where you are.
I wish to leave you with the words of the psychiatrist, philosopher and revolutionary, Dr Frantz Omar Fanon. After working for a couple of years at Algeria’s Blida-Joinville psychiatry hospital, Fanon realised that the revolutionary treatment methods he had introduced on the Algerian victims of French imperialist violence, were an exercise in futility.
He then decided to resign from the practice of psychiatry to join the armed wing of Algeria’s National Liberation Front (FLN). In his resignation letter to the minister concerned, Fanon made a profound observation and said:
The function of a social structure is to set up institutions to serve man's needs. A society that drives its members to desperate solutions is a non-viable society, a society to be replaced.
Camagu!
For counselling queries e-mail: zane@sadag.org
To contact a counsellor between 8am-8pm Monday to Sunday,
Call: 011 234 4837 / Fax number: 011 234 8182
For a suicidal Emergency call: 0800 567 567
24hr Helpline 0800 12 13 14
Facebook: The South African Depression and Anxiety Group
Selected references
- Africa Check: 5 Facts Suicide in South Africa
- FACTSHEET: The state of South Africa’s prisons
- Fanon, F (1967). Toward the African Revolution. Translated by Haakon Chevalier. New York: Grove.
- South Africa Unemployment Rate
- Suicide Rate By Country 2018
- Depression
- Depression: let’s talk
- The World Bank In South Africa
- Double life sentences for Farmer's killers